Hypoxia Signaling: HIF1-alpha & HIF2-alpha Recombinant Rabbit Monoclonal Antibodies
The hypoxic response pathway is triggered by low levels of oxygen in the cellular environment. Hypoxia inducible transcription factor (HIF) is central to the hypoxic response. HIF exists as a heterodimeric transcription factor composed of an alpha and beta subunit. In mammals there are three HIF-alpha subunits, HIF1-alpha, HIF2-alpha, and HIF3-alpha, and one beta subunit, the aryl hydrocarbon receptor nuclear translocator (ARNT). The overexpression of HIF1-alpha and HIF2-alpha is associated with poor survival rates for various cancers. Experimental and clinical evidence strongly suggests HIF1-alpha and HIF2-alpha influence tumor development and response to treatment. Because of this, there has been major interest in developing selective HIF inhibitors; but due to the complexity of the HIF pathway, the process has been challenging. Thus, future work for therapeutic targeting of the HIFs will require a better understanding of both the HIF1-alpha and HIF2-alpha pathways.
Bethyl has expanded its capabilities and now offers rabbit recombinant monoclonal antibodies to HIF1-alpha and HIF2-alpha. These antibodies are available as a trial size (marked in the catalog ending in "-T") and have been validated for multiple applications.
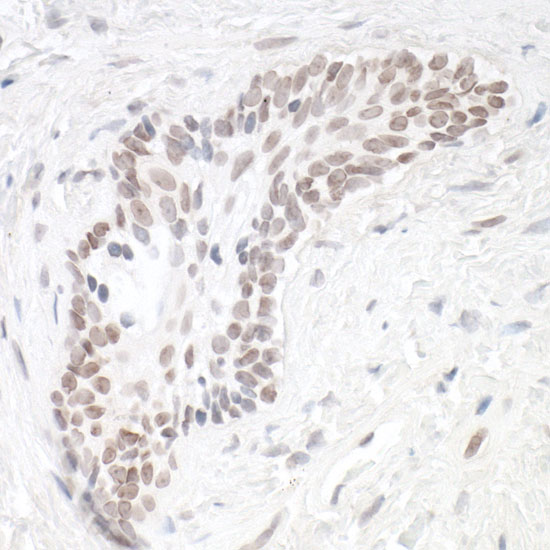
Detection of human HIF1-alpha in FFPE renal cell carcinoma by IHC. Antibody: Rabbit anti-HIF1-alpha recombinant monoclonal [BL-124-3F7] (A700-001). Secondary: HRP-conjugated goat anti-rabbit IgG (A120-501P). Substrate: DAB.
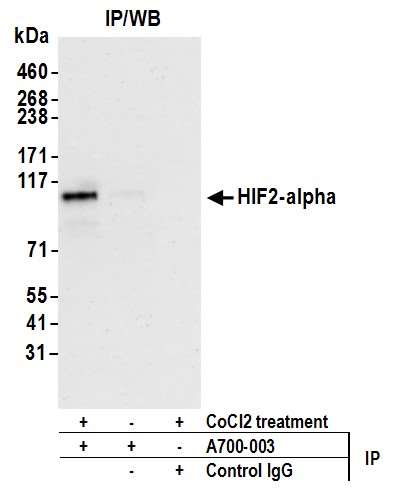
Detection of human HIF2-alpha by WB of immunoprecipitates from HEPG2 lysate treated with 200 µM CoCl2 (+) or mock treated (-). Antibody: Rabbit anti-HIF2-alpha recombinant monoclonal [BL-95-1A2] (A700-003). Secondary: ReliaBLOT® reagents (WB120).
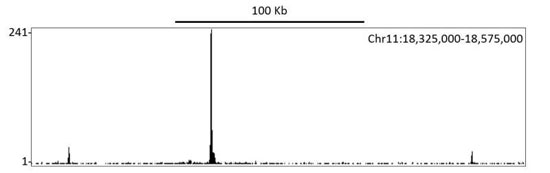
Localization of human HIF1-alpha binding sites in immunoprecipitates from CoCl2 treated HepG2 lysates by ChIP-Seq. Antibody: Rabbit anti-HIF1-alpha recombinant monoclonal [BL-124-3F7] (A700-001).
Bethyl's Comparison
Antibodies against HIF2-alpha were assessed for specificity by immunocytochemistry (ICC). HIF2-alpha protein is rapidly degraded under normoxic conditions and stabilized under hypoxic conditions. Cobalt chloride treatment can be used as a mimetic agent for hypoxia to stimulate HIF2-alpha stabilization. Antibodies against HIF2-alpha were compared by staining HepG2 cells treated with cobalt chloride or mock-treated.
The antibodies included a Bethyl recombinant rabbit monoclonal antibody (Catalog #A700-003), a widely available mouse monoclonal, clone EP190b, from Competitor A, and a goat polyclonal from Competitor B. As expected, in untreated cells, no staining was observed for all antibodies except the Competitor B goat polyclonal, which exhibited off-target nuclear staining. In treated cells, upregulated, nuclear localized, HIF2-alpha was correctly detected by Bethyls Cat#A700-003. This was in contrast to Competitor A's antibody which detected an upregulated protein incorrectly localized to the cytoplasm, and Competitor B's antibody which detected no change in response to treatment.
*All antibodies were tested as per supplier datasheets.
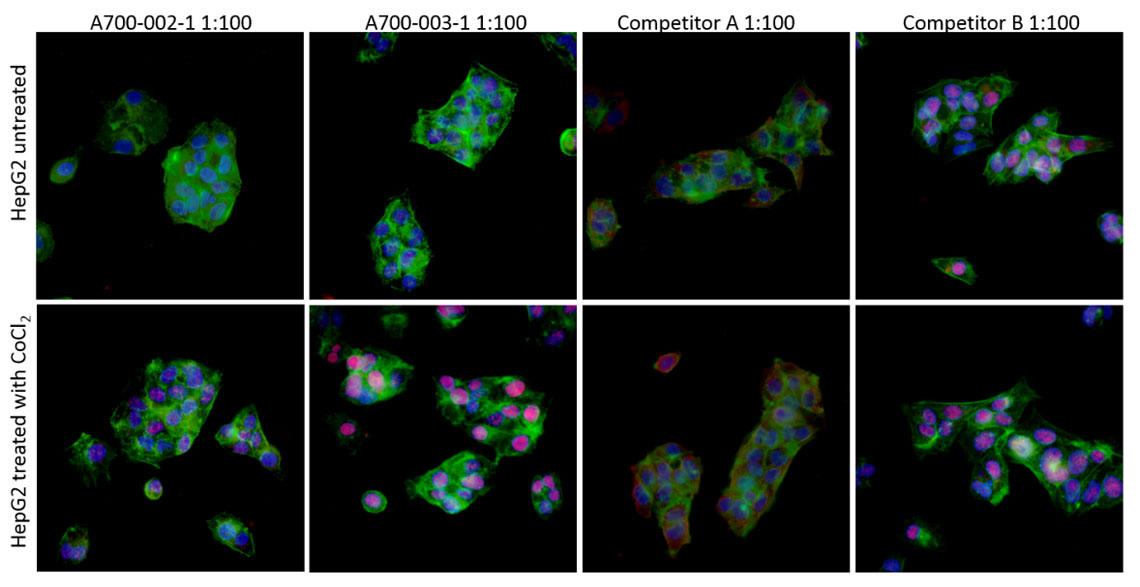
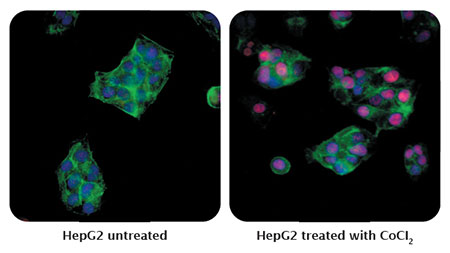
Detection of human HIF2-alpha (red) in formaldehyde-fixed asynchronous HepG2 cells untreated (left) and treated with CoCI2 (right) by ICC-IF. Antibody: Rabbit anti-HIF2-alpha recombinant monoclonal [BL-95-1A2] (A700-003). Secondary: DyLight® 594-conjugated goat anti-rabbit IgG (A120-201D4). Counterstain: DAPI (blue).