Molecular Abnormalities in Breast Cancer
Sex hormones – estrogen in particular – are strongly implicated in breast cancer. Mutations in a number of genes such as BRCA1/2 that confer risk for the disease are thought to lead to elevated levels of estrogen and progesterone1. Increased exposure to estrogen and progestierone through the use of hormonal birth control is also associated with a higher risk for the disease2. Breast cancers are primarily classified by the presence or absence of estrogen receptor, progesterone receptor, and the non-hormone-related molecule human epidermal growth factor receptor 2 (HER2). Therapies targeting these receptors are among the most common treatments for the disease.
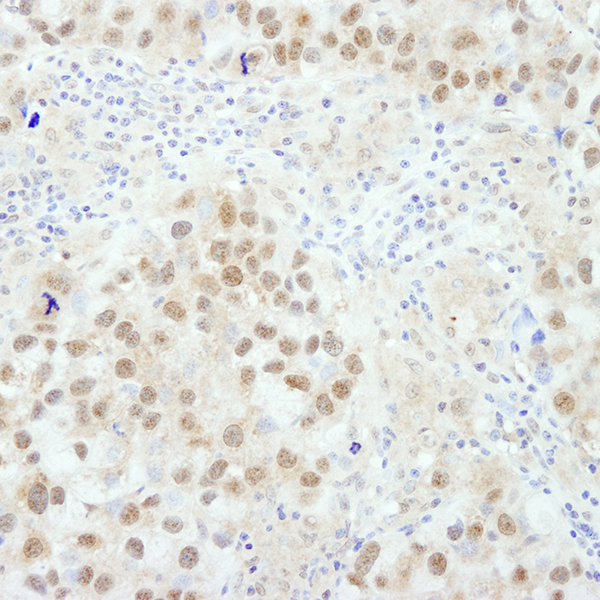
Detection of human BRC1 in FFPE breast carcinoma by IHC. Antibody: Rabbit anti-BRC1 (IHC-00278). Secondary: HRP-conjugated goat anti-rabbit IgG (A120-501P). Substrate: DAB.
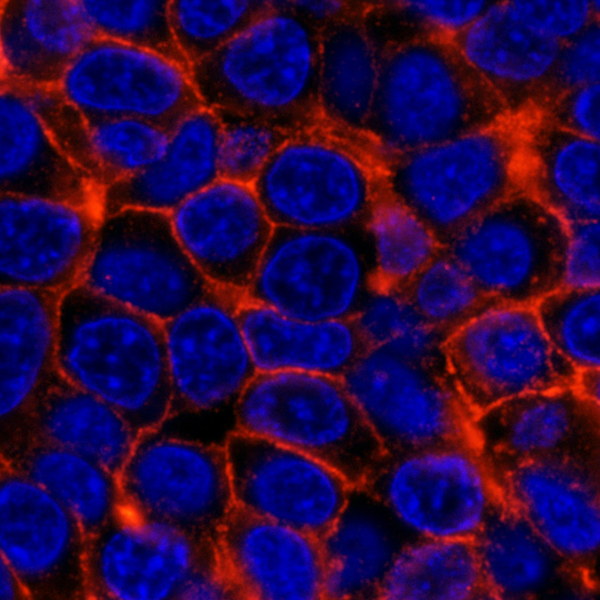
Detection of human ErbB2 (red), commonly referred to as HER2, in FFPE human breast carcinoma by IHC-IF. Antibody: Rabbit anti-ErbB2 (IHC-00032). Secondary: DyLight® 594-conjugated goat anti-rabbit IgG (A120-201D4). Counterstain: DAPI (blue).